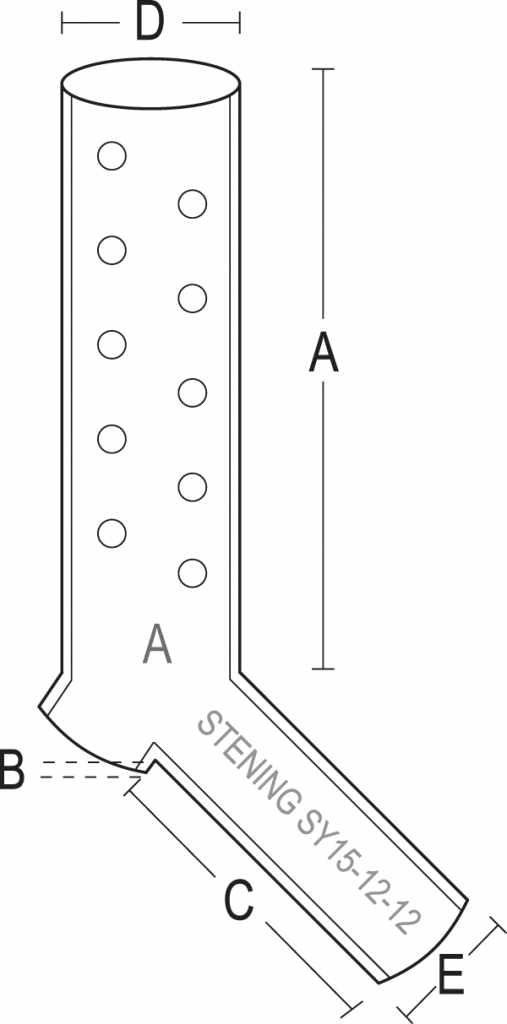
Available dimensions
The Stening® Y Occlusive is offered in two diameters (15 and 16 mm). Measurements A, B, C, D and E (in millimeters) correspond to the references in the diagram.
| Code | Diameter | A | B | C | D | E |
|---|
| SYO15-12 | 15 | 70 | 3 | 30 | 15 | 12 |
| SYO16-13 | 16 | 70 | 3 | 35 | 16 | 13 |
Measurements expressed in millimeters. For specific inquiries about sizes, instruments, bronchoscopes or introducers, contact us at (+54) 11 4553-5070 or (+54) 11 4551-2333.
Implantation
The procedure is performed under general anesthesia. The implantation of this type of prosthesis must be carried out by experienced personnel. The stent can be mounted on a special forceps for the implantation of “Y” prostheses.
Lubricate the tip of the forceps with lidocaine gel. Insert the forceps into the stent so that its jaws penetrate the interior of the prosthesis’ bronchial branches. Ventilate the patient with oxygen until reaching the highest possible saturation. Then extubate, withdrawing the tracheoscope from the airway. Immediately, and with the help of a laryngoscope, guide the forceps holding the stent toward the trachea. When the jaws of the forceps are closed, the bronchial branches of the stent come together, and in this position the stent passes between the vocal cords into the trachea. The maneuver continues by advancing the forceps-stent assembly within the trachea until approaching the carina.
When the end of the forceps-stent assembly is near the tracheal carina, the jaws of the forceps must be gently opened in order to perceive the arrival of the prosthesis at the tracheal bifurcation. At this moment the jaws are fully opened so that the bronchial branches of the stent are introduced into the main bronchi. Then the forceps button is pressed, holding the stent against the carinal edge, while the forceps is withdrawn. The whole maneuver must be quick, since it is performed with the patient extubated and in apnea.
We recommend using direct-vision optics to ensure that the stent passes the vocal cords and is not accidentally led toward the esophagus. To this end, the optics must accompany the forceps maneuver in parallel, allowing one to see and confirm that the stent enters through the glottis. This option is only possible with the help of a second operator, who keeps the intubation laryngoscope in the proper position while the bronchoscopist uses the dominant hand for the stent insertion forceps and the other to hold the optics. Other implantation techniques are possible, such as introducing the folded prosthesis inside a bronchoscope of sufficient caliber, then pushing it through its interior with an alligator forceps or a smaller-diameter bronchoscope, once it is near the tracheal carina. The implantation maneuver can be completed by adjusting the prosthesis with a forceps.
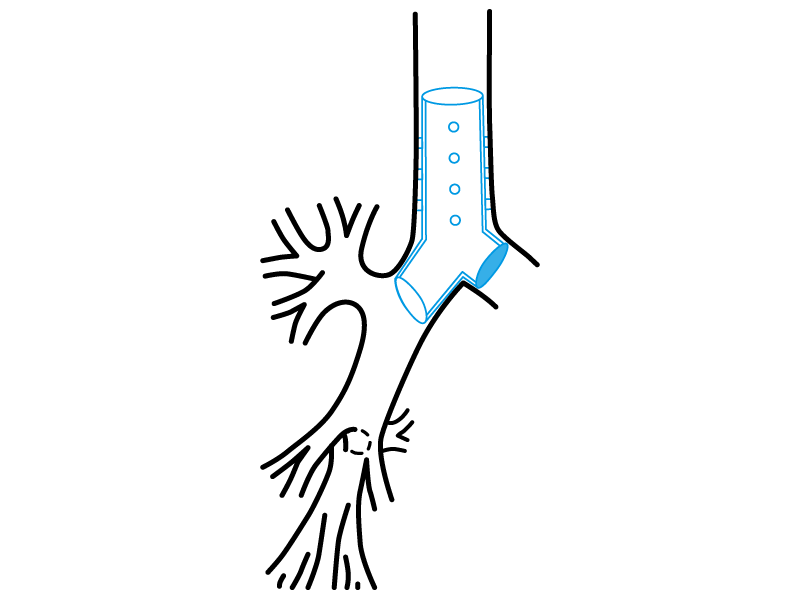
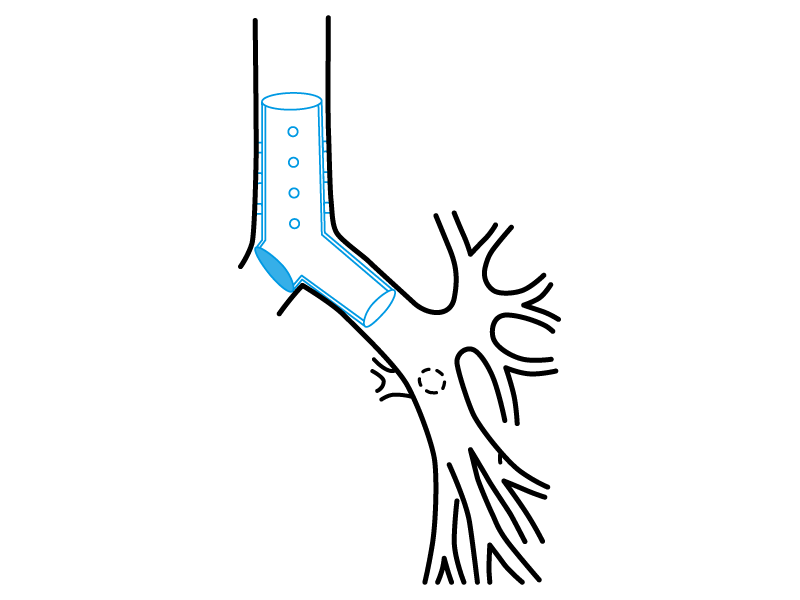
The use of a special forceps for introducing “Y” stents is not essential, since this device has only one bronchial branch. The implant is then carried out by introducing the stent inside a tracheoscope, and then intubating the airway with the assembly. When loading the stent inside the endoscope, the bronchial branch must be oriented in the direction that allows it to occupy the affected main bronchus or stump in the airway.
Once the patient is intubated, advance within the trachea until approaching the carina. The stent is then pushed with a forceps, in order to force it to leave the tracheoscope and become lodged in the trachea. The final position can be adjusted with the same forceps, so that the single bronchial branch of the stent is lodged inside the chosen main bronchus.
Removal
Intubation is performed with a tracheoscope. Removal is simpler: the stent must be grasped by its proximal edge with strong forceps and withdrawn gently by pulling on it, extracting the prosthesis together with the tracheoscope.
Post-implant care
Recommendations for the follow-up of the patient with an occlusive Y stent.
The application of this device implies a critical patient condition, usually under respiratory support in an intensive care unit. Therefore, care of the stent consists of performing frequent aspirations and humidifying the supplied airflow, in order to dilute secretions and prevent their accumulation.