Abstract
The paper describes two new endoscopic signs which can be useful in the use of diagnostic bronchoscopy. This is an essay on particular anatomic and functional circumstances suggesting the presence of a pathology which cannot be seen by the bronchoscopist. These two signs are the Bubble Sign and the Black Hole Sign. The Bubble Sign is observed when the airflow is absent in a subsegmental bronchus leading to a peripheral pulmonary mass. This can be shown by the lack of mobile bubbles when a subsegmental bronchus is flooded with saline solution. The Black Hole Sign consists in the circular penumbra observed at the end of a bronchus which communicates with a cavity.
The paper describes the presentation and interpretation of these signs and offers an explanation about their physiopathology.
Key words: Bronchial fistula – bronchial neoplasia – bronchoscopic signs
Bubble Sign
Definition
In the bronchus that leads to a peripheral pulmonary mass, the airflow is absent, and this is verified by the lack of bubbles in movement when flooding it with saline solution.
The bubble sign is the “absence of bubble formation” after instilling the saline solution, and it indicates the existence of a distal obstruction in that bronchus.
Usefulness
The bronchoscopic examination is a frequent practice in patients with peripheral pulmonary opacities. Few endoscopic signs have been described1, and it is common for the endoluminal repercussion findings of this pathology to be absent. When a carcinoma is suspected, different techniques, such as transbronchial lung biopsies, brushings or cryoprobes, are used to obtain the diagnosis2, 3.
These lesions that occlude the bronchus totally or partially also stop the airflow in that bronchus4, 5. When the obstruction of a bronchus is peripheral, it is not visible to the bronchoscopist, and the presence of this sign can be useful to identify the affected bronchus.
In the “bubble sign”, a phenomenon then develops that allows the bronchoscopist to identify the bronchus that leads to a pulmonary mass; that is, the bronchus affected by that pulmonary mass, but which is obstructed beyond the bronchoscopist's possibilities of observation, and thus to select the bronchial orifice through which the biopsy forceps, the cytological brush or the cryobiopsy probe must be introduced.
Pathophysiology
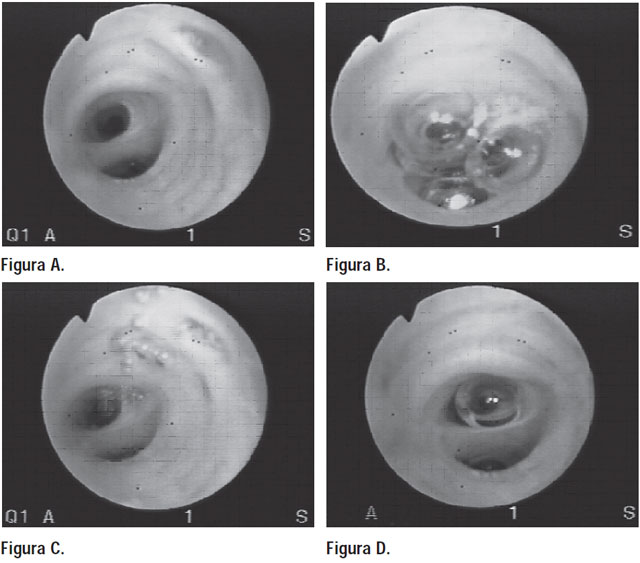
In a pulmonary mass in which the parenchyma has been totally or partially replaced by neoplastic tissue, ventilation will be absent or at least diminished, and its access bronchus occluded. Even so, since it is a peripheral bronchus, the inspection of the segmental, subsegmental and even the 4th-order bronchi that constitute the limit of the bronchoscopist's exploration will be completely normal on visual examination (Fig. A).
However, the airflow in the bronchus will be absent due to its distal obstruction. The lack of air circulation can easily be evidenced by instilling about 20 milliliters of saline solution into the lobar or segmental bronchus.
The instilled physiological solution replaces the air due to its greater weight and combines rapidly with it, forming a “rosary” of small moving bubbles (Fig. B) that circulate along the normal segmental and subsegmental bronchi as a result of the respiratory movements. This phenomenon will be absent in the access bronchus to the tumor when it is obstructed at a site far from the possibilities of observation (Fig. C).
The absence of this hydroaerial rosary constitutes the “bubble sign” (Fig. D).
When dealing with bronchi with posterior courses –as occurs with the apical bronchus of the lower lobe– and with the patient in the dorsal decubitus position, even after aspirating the solution, the remaining liquid combines with secretions and accumulates again at the entrance of the apical bronchus, by gravity, “refilling” it, since its distal obstruction does not allow the passage of the solution to the lung tissue, as occurs in normal bronchi.
The bubble sign may be present in conditions as frequent as radiological opacities due to lung tumors, in which the absence of endoscopic findings constitutes a challenge for the bronchoscopist. The instillation of saline solution is a maneuver that reveals a distal obstruction in a simple way and does not add time or complications to the examination. The bubble sign makes it possible to easily choose the segmental bronchus that leads to the affected bronchus, in order to then introduce the instrument for the biopsy.
On occasion, the operator may “feel in their fingers” the stop to the advance of the biopsy forceps or the cytological brush, and thus recognize that the selection of the bronchus has been correct.
The capture of tissue samples performed, guided by the bubble sign, was initially very encouraging by virtue of the diagnostic confirmation obtained in the first cases examined. The numerical expression of its effectiveness will need to be known, comparing it with the conventional biopsy guided by imaging and fluoroscopy, in addition to the always-present intuition of the operator; as well as the diagnostic certainty of the biopsies taken in the bronchi that have a positive bubble sign, compared in turn with the samples obtained in the adjacent bronchi, but without the bubble sign present.
The need to extend the study of this semiological tool thus remains pending.
No changes were observed in subsequent follow-ups; the patient remained asymptomatic and was ultimately considered cured.
Black Hole Sign
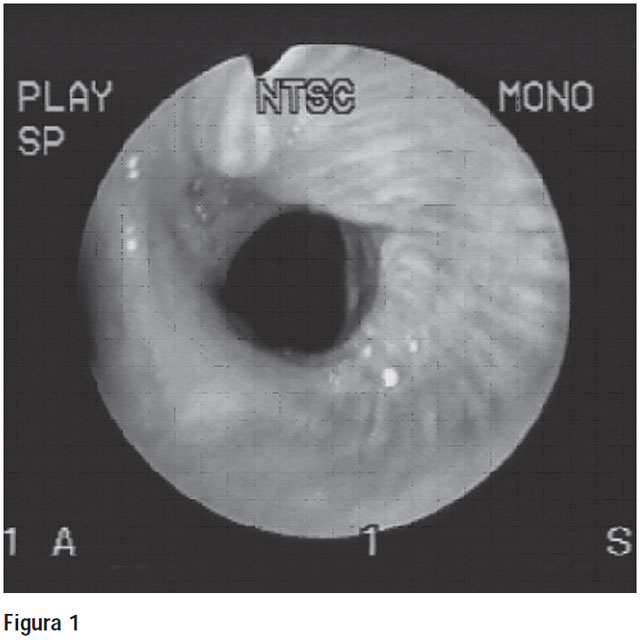
It is the circular penumbra seen at the end of a bronchus when it communicates with a cavity (Figure 1).
Description
The endoscopic exploration of the bronchial tree offers the operator a journey through the airway, with an almost circular lumen, variable lengths and progressively smaller diameters. The bronchial tree can thus be traversed with its pink-colored mucosa, towards the more distant divisions, segmental and subsegmental, less illuminated but of the same color.
The “black hole sign” is the completely dark or circular appearance of the bronchial lumen, compared to the usual color of the illuminated mucosa.
The black hole sign is present when the bronchus being explored communicates with a cavity or when it presents a saccular dilation. Therefore it can be found in segmental and subsegmental bronchi, but it can also be found in lobar bronchi, as occurs in the bronchopleural fistula that appears as a complication of lobectomy.
The reasons that make its appearance possible are simple, and to understand them we must consider the bronchus in its morphology, comparable to the section of a cone6, (Fig. E), in which its diameter decreases as we progress through its interior. The flexible bronchoscope emits a light that propagates in a parallel and divergent way (Fig. F), and illuminates the bronchial walls.
The beam of rays will be refracted and reflected according to its angles of incidence (Fig. G), and will contribute to the distal illumination77.
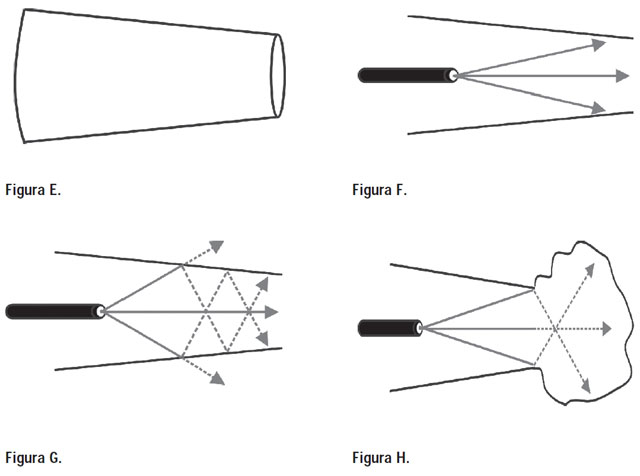
When a bronchus is dilated from a point of its course, or when it communicates with a cavity, its conical structure is lost or modified. The light emitted by the source is insufficient to reach the cavity walls (Fig. H). The final result is the low luminance of the dilated bronchial walls or of the cavity.
The bronchoscopist will observe, among all the pink bronchial bifurcations, one with the appearance of a dark circle due to the existing distal penumbra.
In image C2, the measurements are taken on devices that have been aged in the laboratory.
References
- López Aráoz A. Broncoscopia para Clínicos y Neumonólogos. Publicaciones Latinoamericanas SRL, primera edición, 2008; 1: 21-22.
- Pajares V, Torrego A, Puzo C, Lerma E, Angels Gil De Bernabe M, Tomá F. Utilización de criosondas para la realización de la biopsia pulmonar transbronquial. Arch Bronconeumol 2010; 46(3): 111-115
- Zafer Aktas, Ersin Gunay, Nevin Taci Hoca et al. Endobronchial cryobiopsy or forceps biopsy for lung cancer diagnosis. Thorac Med 2010; 5(4): 242-246.doi: 10.4103/1817- 1737.69117.
- Soulas A, Mounier – Kuhn P. Bronchologie. Editorial Masson et. Cie., 6ta edición, 1956; tomo I, capítulo 9: 235-240.
- Fraser RS, PARE PD. Diagnóstico de las Enfermedades del Torax. Editorial Panamericana, Cuarta edición 2002; Vol II: 1080-1116.
- Castella J, Puzo C. Broncologia. Editorial Salvat Editores SA 1982; 1: 1-5.
- Tipler PA. Física Preuniversitaria. Editorial Reverte S A, versión española, 1992; 24: 715-719.