Clinical case
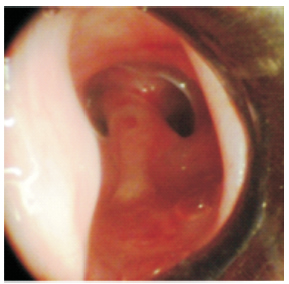
A 20-year-old male was treated in the intensive care unit due to polytrauma resulting from a traffic accident. He received mechanical ventilation for 11 days through an orotracheal tube. Three weeks later he presented obstructive respiratory distress and underwent tracheostomy. A flexible bronchoscopy showed, 1.5 cm from the vocal cords (Figure 1), the existence of a thick sagittal septum of tissue dividing the trachea into two channels (Figure 2).
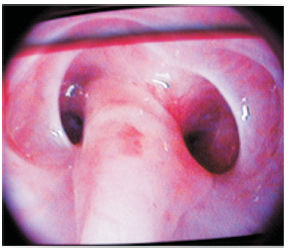
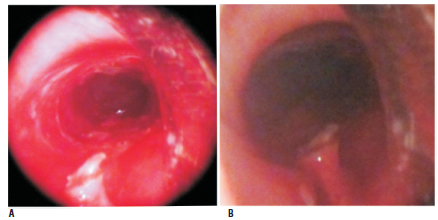
This anomaly was arranged between the anterior and posterior walls of the trachea and extended in a cephalocaudal direction for about 3 cm, ending near the tracheal stoma. At the same time, both resulting channels maintained a reduction of the lumen due to circumferential fibrous stenosis. Each channel had an approximate diameter of 5 millimeters and they coincided in the axial plane. A rigid bronchoscopy was performed under general anesthesia and the septum was resected along its entire length with an electrocautery snare, followed by mechanical dilation with the bronchoscope, which resulted in complete recovery of the tracheal lumen (Figure 3a). A number 12 T-tube was placed through the tracheostomy orifice to ensure tracheal stability. The device was removed after 12 weeks, with recovery of the lumen and re-epithelialization of the tracheal mucosa; the persistence of a small remnant of the septum on the posterior wall was observed (Figure 3b), which did not require treatment. The patient remained asymptomatic and was discharged.
Discussion
There are reports about the existence of thin, transverse fibrotic bands of subglottic location and variable course1-3. They in no way resemble what is reported here and were described as a consequence of systemic inflammatory processes, laryngeal trauma, or as congenital findings. Wegener's granulomatosis may be accompanied by subglottic stenosis4 or arches of fibrous tissue located in the larynx. This systemic small-vessel vasculitis has a predilection for the upper respiratory tract. The usual involvement of the larynx consists of a concentric subglottic stenosis, which occurs in 9 to 23% of cases5. Although biopsy of the stenosis offers a low percentage of diagnostic compatibility, biopsies of the nasal mucosa have shown 82% sensitivity for Wegener's granulomatosis in patients who have antineutrophil cytoplasmic antibodies. In the sources consulted, no reports of complete tracheal septations were found. The presence of this anatomical anomaly of curious configuration challenges the bronchoscopist to reflect on some possible causal mechanisms, or at least one. The history of orotracheal intubation suggests the possibility of an inflammatory process from which a stenosis may derive; however, what was found and described in no way resembles the usual narrowings. Circumferential inflammation does not seem to be a reason for the swollen mucosa to extend, at two diametrically opposite points, toward the opposite wall until it comes into contact with it and joins to form a septum. Even more remote would be the possibility that the septum had originated from a single point of the inflamed tracheal perimeter. Another possible mechanism requires the existence of a scalp of the tracheal mucosa, which may well have originated during the maneuvers of orotracheal intubation or extubation, by the end of the tube or by its fixation cuff, thus leaving a flap of tissue that, suspended from the upper wall, came into contact with the lower one, which was highly inflamed, and joined it to form a septum. Careful endoscopic evaluation followed by endosurgical resection with the implantation of a T-tube was effective in restoring the tracheal lumen in this case.
Conflicts of interest
The authors declare that they have no conflicts of interest.
References
- Christopher M, Stafford MD, James H, et al. Subglottic web treated with Nd YAG laser. Bronchology 2003; 10, 2: 144-5.
- Rbhun JA. Subglotic web in asthmatic patient. Ann Allergy 1988; 60: 513-4.
- Ballenger J. Subglottic lesions. In: Otorhinolaryngology Head and Neck Surgery. Baltimore: Williams & Wilkins, 1996, pp 509-13.
- Herridge MS, Pearson FG, Downey GP. Subglottic stenosis complicating Wegener's granulomatosis: surgical repair as a viable treatment option. J Thorac Cardiovasc Sur 1996; 111: 961-6.
- Seo P. Wegener's granulomatosis: managing more than inflammation. Curr Opin Rheumatol 2008; 20(1): 10.