Endoscopic Center, Hospital Enrique Tornú, Buenos Aires, Argentina
Introduction
Tracheobronchial prostheses are used to treat obstruction of the large airway in benign conditions and to palliate the effects of obstruction caused by neoplastic lung disease.
In the last 20 years a great variety of stents have been used for this purpose, until in 1990 Dumon published the results of his experience with a new model of silicone prosthesis. Since then, it has been the most widely used stent in the world(1-2-3-4-5-6-11-12).
The treatments performed mostly require a procedure of recanalization or "reconstruction" of the tracheal or bronchial lumen, often followed by the insertion of a prosthesis to ensure airway support. The use of silicone stents is also widespread in our setting. This is largely due to the great experience and prolonged case series already existing and, to a good extent, because it is a safe device that is simple to apply and remove.
Material and method
Silicone prostheses made of polysiloxane have been used, which have shown great tolerance as a result of their elastic properties(7-10). The dimensions of the stent were determined by performing a fiberoptic bronchoscopic examination prior to the interventional procedure. In this way, the possible measurements required for its insertion were estimated. The prostheses, in turn, were available in progressive calibers from 5 mm, and in variable lengths. On certain occasions, the stent was subjected to modifications consisting of adapting the length and termination angle of the bronchial branches. This applies to "Y" prostheses, in the particular cases in which it was necessary to maintain ventilation of the right upper lobe, when it originates from a short main bronchus.
The ends of the prosthesis must have a smooth finish, in order to achieve continuity with the bronchial mucosa without provoking the appearance of inflammatory phenomena.
The airway disobstruction procedures were performed with a high-frequency electrosurgical unit(12). All of them under general anesthesia, with monitoring of the inspired fraction of O2 and exhaled carbon dioxide. Even so, no risk of combustion was possible, since ventilation was carried out with compressed air. In the benign stenoses, mechanical dilation was performed(8), with or without complementary resection with electrocautery.
Occlusive and subocclusive lesions, of benign or malignant nature, of the trachea and/or bronchi were treated in 50 patients. All of them had been excluded from conventional open surgery because of the anatomical characteristics of their lesions or due to the advanced stage of their disease.
Implantation
The prosthesis to be inserted is lubricated with lidocaine gel, folded on its axial axis and introduced into the interior of the prosthesis loader, through the nozzle provided for this purpose. The assembly is thus introduced through the rigid bronchoscope, which will be in the appropriate position to release the stent inside the area treated for the stenosis.
Complete expansion requires, in some cases, maneuvers to complete the opening of the stent, with a forceps with toothed jaws, of the alligator type.
Deformations in the implanted stent were not taken into account when they did not affect more than 20% of its circumference. The recomposition of the circular lumen was always spontaneous in these cases, requiring for this a period of between 48 hours and 7 days.
The Y tracheobronchial prostheses were implanted with a forceps capable of mounting it on the outside, with both bronchial branches folded. It was thus introduced through the glottis, visualized with an orotracheal-intubation laryngoscope. This function can be performed very well by the Storz forceps for dynamic stents and was used in 3 cases. Other forms of implanting Y prostheses are possible and perhaps simpler, depending on the experience of each operator.
Removal
To extract the stent, it is grasped by its proximal edge with the alligator forceps, firmly enough. A rotation movement produces the collapse of the stent, with reduction of its diameters and separation from the tracheobronchial mucosa. When the forceps is pulled, it is extracted together with the bronchoscope. The same procedure is useful for removing "Y" prostheses.
Results
Patients
Between March 15, 1999, and the 15th of the same month of 2002, 60 silicone prostheses were used to treat 50 patients with benign or malignant lesions involving the trachea, carina, main or intermediate bronchi, separately or in combination, and which produced partial or total occlusion of the airway.
The group of patients consisted of 23 women and 27 men, in an age range from 14 to 85 years, with a general average of 50.2 years.
Twenty-two of them presented benign tracheal stenosis, with an exceptional case of single involvement of the left main bronchus, also of the benign stenosis type.
All cases, with the exception of one, had a clear history of tracheal intubation, sometimes as brief as 72 hours.
The histological diagnoses of the malignant conditions, in a total of 28 cases, were: 12 adenocarcinomas, 6 squamous, 3 small-cell carcinomas, 2 undifferentiated, and another two could only be identified as carcinoma.
One case corresponded to the invasion of the tracheal lumen by thyroid carcinoma. A bronchial obstruction with carinal invasion by metastasis of clear-cell renal carcinoma was also treated. Finally, an infrequent loss of the tracheal cartilaginous support due to actinic necrosis of this organ, in a patient undergoing radiation therapy for an epidermoid carcinoma of the right upper lobe.
Type of prosthesis and location
Twelve "Y" tracheobronchial stents were used, all of them in the measurement of 15 mm tracheal diameter and 12 millimeters for each of the bronchial branches. Their lengths, as well as those of their tracheal portion, were adjusted, in each case, to the affected distance in the airway, bearing in mind that no stent should be longer than necessary. Thus, the necessary section of the prosthesis was always followed by the abrasion of its edges in order to eliminate sharp angles in the material that could impinge on the mucosa. This is how the sectioned branch acquires the original conformation.
The rest of the prostheses were 21 bronchial and 27 tracheal which, being supplied in the necessary measurements, never needed to be shortened.
The greater number of stents than of patients is explained by the fact that some of them required more than one prosthesis during their treatment, due to local progression of the neoplastic disease, from the main bronchus to the carina or toward the trachea. Other stents were replaced at 12 months due to hypersecretion and encrustation.
A single case with adenocarcinoma was treated with two prostheses, one in the right main bronchus and another implanted four months later in the distal trachea, due to progression of the disease.
The insertion of bronchial prostheses was performed in the left main bronchus in 12 cases, in the right in 9 and in the intermediate bronchus in 2.

Complications
The description of the complications will be brief, since these were comparatively low(6).
Hypersecretion was the most frequent manifestation and occurred in 5 cases (8.3%). The patients performed nebulizations with saline solution as frequently as at 4-hour intervals, without this resolving the increase in the amount of secretions.
Aspirations were then performed with a fiberoptic bronchoscope, with special interest in removing the secretions that might be adhered to the inner wall of the stent. They become consistent due to the dehydration that derives from the increase in the speed of the air flow in the prosthesis, which has a smaller caliber than the airway itself in the same path. When their removal was not satisfactory, the prosthesis was extracted and replaced.
In one case (1.6%), colonization of the stent by Candida albicans was demonstrated one year after its insertion, and it was also replaced.
The development of a granuloma on the free edge of a tracheal stent implanted as a consequence of a benign stenosis was observed in a single case (1.6%).
As for migration, it only occurred in 3 cases (5%), all of them corresponding to benign stenosis in which the mucosal surface, much more regular than in neoplastic infiltration, reduces the possibilities of stent fixation.
Compression of the prosthesis by tumor growth was not observed in any case. This is easily explained by the pressure-support capabilities offered by the prosthesis wall, which is between 800 and 1000 grams per square centimeter. Occlusion of the stent by growth of the neoplasm was not observed either.

Case reports
Case 1
A 50-year-old woman consulted for hemoptoic expectoration. Her chest X-ray was normal. The bronchofibroscopic examination demonstrated the presence of a formation that occluded 90% of the lumen of the left main bronchus, sitting 1 cm from the carinal edge. The lesion corresponded to an adenocarcinoma and was resected with electrocautery. A 12 x 35 stent was implanted at that level.
One year later, the prosthesis presented encrustation of whitish secretions firmly adhered to the inner wall. Its study demonstrated the presence of Candida albicans. The stent, which showed little useful section for ventilation, was extracted and replaced.
Fourteen months later, secretions fixed to the wall of the prosthesis were found and the stent was replaced again, although the cultures were negative.
The following year, an expiratory wheeze was audible in the center of the chest; an endoscopic examination was indicated, with the suspicion of stent subocclusion. The study made it possible to determine that the lumen of the prosthesis was normal; however, the advance of the disease was causing the intramural infiltration of the wall of the contralateral main bronchus, with a notable reduction of the lumen that originated the wheeze. The carinal edge was distorted and the extraction of the left main bronchus stent was indicated, for its replacement with a carino-bronchial "Y" prosthesis.
At present, the patient's survival has exceeded 40 months.
Case 2
A 45-year-old woman was referred to the service for atelectasis of the left lung. Eight years before her admission, she had undergone a left nephrectomy for clear-cell carcinoma. The same histological diagnosis was obtained after examination of the biopsy specimen from the formation that totally occluded the lumen of the left main bronchus, in the vicinity of the carina.
Prosthesis implantation was not performed until 10 months later, when significant local recurrence of the tumor was found, along with submucosal miliary nodules on the slopes of the carina. A Y stent was used that had to be extracted a few days later due to intractable coughing, and replaced with a 13 x 35 bronchial prosthesis, which was implanted in such a way that its proximal end exceeded the carinal edge.
New tumor recurrences appeared with a distal bronchial location, occluding the lingula and the upper lobe, which were treated with electrocautery through the channel of the fiberscope, which was introduced through the stent, without it being necessary to remove it to vaporize the lesion. Successive treatment sessions were carried out until her death, 24 months after her first admission to the hospital.
Case 3
A 71-year-old man is admitted to the Intensive Care Unit for severe respiratory distress, which required orotracheal intubation, without mechanical ventilation.
The patient carried an epidermoid carcinoma of the right upper lobe which, being considered stage IIIB, received radiation treatment consisting of 6000 centigray over a field of 11.5 x 12 cm on the chest.
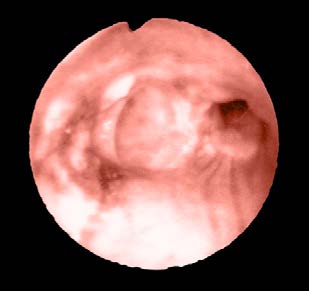
The tracheal tube was removed and an endoscopic examination revealed the complete loss of the cartilaginous support of the intrathoracic trachea, with exposure of the rings. Image 2a
Inspiration was followed by incomplete collapse of the wall, and many of the ends of the rings were "free" in the lumen. Purulent secretions lined a large part of the mucosa, whose biopsy indicated tissue necrosis.
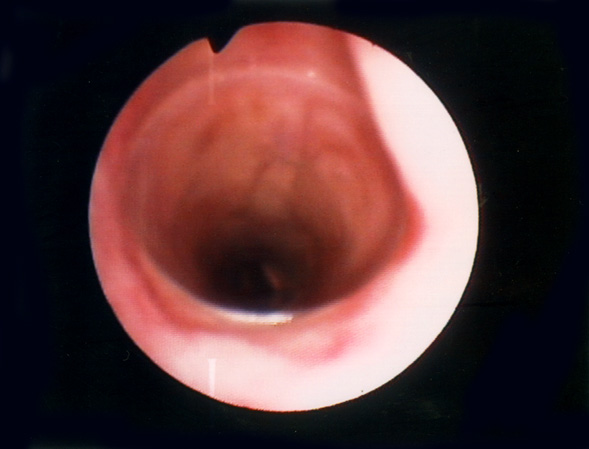
A 16 x 70 millimeter silicone stent was inserted. It expanded so rapidly that its replacement with another of 17 x 70 mm was considered necessary. The destruction of the tracheal rings or their separation from the fibroelastic sheath makes the trachea "compliant", and a stent can thus expand comfortably(9); in any case, the exposure of the cartilaginous arches resulted in an excellent fixation of the stent in them. The maneuver made it possible to recover the tracheal lumen and keep the patient breathing spontaneously. Image 2b

Discussion
The usefulness of a stent to maintain the patency of the airway seems beyond all doubt.
The recurrence of benign stenosis, after recanalization treatment by any endoscopic method, is variable, and its immediate recurrence is prevented by the prosthesis. On the other hand, tracheal or bronchial resection and disobstruction, followed by radiation treatment or chemotherapy, may be sufficient in some cases, and the application of a stent immediately after recanalization could be questioned. However, the absence of reports about prosthesis obstruction due to proliferation of neoplastic tissue makes its early use a safe way to maintain ventilation through it and saves a second future intervention to implant the prosthesis.
Although in all these cases it is accepted that its indication has a palliative purpose closely linked to quality of life, especially when it is a carino-bronchial stent, long survivals such as those we have presented can be found in many published series(2-3-11).
The use of two prostheses to cover affected areas such as the main bronchus and distal trachea, when the carina and the contralateral main bronchus remain intact, turned out to be preferred over the use of a "Y" stent. The reason is that the entire path of the stent that exceeds what is necessary to cover the condition being treated should be considered a "foreign body". As such, the dependent effects such as interference with the ciliary sweep, excessive rigidity, reduction of the lumen, and greater impaction of secretions, to mention only a few, should be taken into account. Therefore, the shorter the necessary stent, the better.
Once again, to the advantages already widely known from the great accumulated experience in the use of silicone prostheses, their drawbacks will be subtracted.
First, the one that has perhaps been least referred to so far will be mentioned: the relatively scarce available lumen, if one takes into account that the wall of the prosthesis occupies between 33 and 36% of the total surface of the stent section(*), or, what is the same, in a silicone prosthesis only 2/3 of its diameter will be destined for the air passage and, what is worse, for the passage of secretions through it. This is consequently related to the frequent retention of these secretions.
As a counterpart to the high wall/lumen ratio, the wall itself is capable of tolerating between 800 and 1000 grams —a difference that depends on the different available models— per square centimeter of its surface without reaching the breaking point of its resistance to compression(**).
This translates in practice into a high tolerance to extrinsic pressures, which is reflected in the lack of reports of treated cases in which the prostheses have lost their functionality due to excessive deformation by compression on their walls and loss of the lumen.
This series presented a low frequency of prosthesis migration after being implanted in benign tracheal stenoses. A frequency that would be even lower if one excludes from the list a case in which the possibilities of displacement of the prosthesis were as many as those of the stent having been inserted "lower" than was actually necessary. This raises a new topic of discussion about how to establish the exact length of affected tracheal mucosa after the dilation maneuvers have been performed.
Indeed, at the start of the procedure one can have a fair impression of the lesional characteristics, as well as of the ring in which they begin. As the intervention progresses, the initial determinations become imprecise, and this can lead to performing an implant at a level that does not totally protect the affected area, or to choosing an excessively long stent.
The widest possible prosthesis has always been chosen to be applied in the lumen achieved with the recanalization maneuvers, and this fact is considered directly responsible for the low frequency of stent migration. Using a prosthesis of smaller diameter is commonly tempting. After its release in the airway, its complete expansion is immediate and the task seems concluded. A migration in these cases is possible.
The choice of a stent of larger diameter promises a laborious expansion within the trachea. It may, on occasion, remain so folded as to adopt a half-moon shape or, worse still, the letter "omega", occupying the entire tracheal lumen and leaving the impression of an "occluded airway". Even so, ventilation through it will be possible. The use of inflatable balloons for the purpose of expanding the stent has not, in our experience, been satisfactory, since the balloon will spontaneously settle into the angle of the prosthesis that is folded in a horseshoe shape. Manual expansion with alligator-type forceps will be very laborious but will be rewarded by good fixation of the stent.
As a guide, when we have achieved a tracheal lumen such that a bronchoscope of 12.4 mm external diameter can be introduced snugly, we use a stent of 13 or 14 millimeters; and when it has been dilated until the introduction of a 14.4 mm external bronchoscope is possible, a stent of 15, or better 16 mm, will be chosen.
(*), (**) Determinations by the author.
References
- Dumon JF, Cavaliere S, Díaz Jimenez JP, et al. Seven-year experience with the Dumon prosthesis. J Bronchol 1996; 3:6-10.
- Cavaliere S, Venuta F, Foccoli P, Tonielli C, La Face B. Endoscopic treatment of malignant airway obstructions in 2008 patients. Chest 1996; 110: 1536-42.
- Dumon JF, Dumon MC. Dumon-Novatech Y-Stents: A Four-Year Experience with 50 tracheobronchial Tumors Involving the Carina. J Bronchol 2000; 7:26-32
- Filler RM, Forte V, Chait P. Tracheobronchial Stenting for the treatment of airway obstruction. J Pediatr Surg 1998;33:304-11.
- Miyazawa T, Arita K. Airway stenting in Japan. Respirology 1998;3:229-34.
- Jantz, MA, Silvestri,GA. Controversy Silicone Stents versus Metal Stents for Management of Benign Tracheobronchial Disease. J Bronchol 2000; 7:177-183.
- Colt HG, Dumon JF. Airway stents: present and future. Clin Chest Med 1995; 16:465-78.
- Lee KW, Im JG, Han JL, Kim TK, Park JH, Yeon KM. Tuberculosis stenosis of the main bronchus: result of treatment with balloons and metallic stents. J Vasc Interv Radiol. 1999; 10:532-8.
- Bolot G, Poupart M, Pignat JC, et al. Self expanding metal stents for the management of bronchial stenosis and bronchomalacia after lung transplantation. Laryngoscope 1998; 108:11230-3.
- Korpela A, Aarnio P, Sariola H, Tormala P, Harjula A. Bioabsorbable self-reinforced plo-L-lactide, metallic and Silicone sents in the management of experimental tracheal stenosis. Chest 1999;115:490-5.
- Díaz-Jimenez JP, Farrero Muñoz E, Martinez Ballarin JI, Kovitz KL, Manresa Presas F. Silicones Stents in the management of obstructive tracheobronchial lesions: 2 –year experience. J Bronchol 1994; 109:626-9.
- Bollinger CT. Airway stents. Semin Respir Crit Care Med 1997; 18:563.70.